![]()
DAILY DIGEST
REPORTING FROM THE 2021
CONSORTIUM OF MULTIPLE SCLEROSIS CENTERS ANNUAL MEETING
THURSDAY, OCTOBER 28
On the Agenda Today
- 8:00 am – 8:45 am: Donald Paty Lecture: Microbiome in Adults and Pediatrics, Emmanuelle Waubant, MD, PhD, Panzacola F/G
- 9:00 am – 12:00 pm: Women in MS: Building Skills for Thriving In Your Career, Carrie Hersch, DO, Chair, Sandlake
- 9:00 am – 12:00 pm: Late-Breaking Science, Corey Ford MD, PhD, Chair, Panzacola F/G
- 12:00 pm: Meeting adjourned. See you in National Harbor, Maryland in June 2022!
In Aging MS Patient Population, Too Little Is Known About Effects of Treatment
Dr. Le Hua’s data of DMT use in older patients with MS show that most had discontinued DMT. (Click on image to enlarge)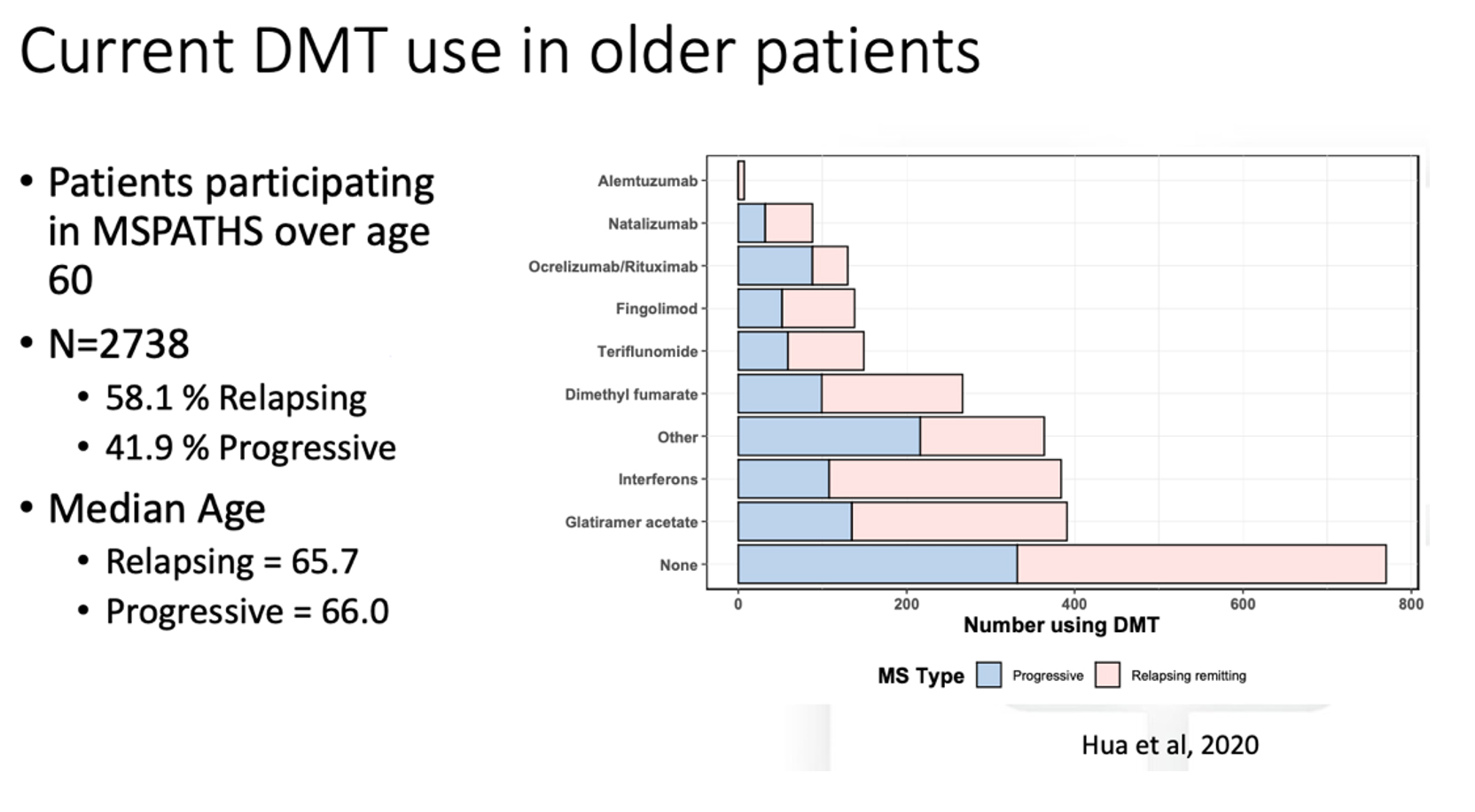
At the CMSC Annual Meeting here, Le Hua, MD, Director of the Mellen Program for MS at Cleveland Clinic’s Lou Ruvo Center for Brain Health in Las Vegas, addressed this dilemma and shared her study findings from the MS PATHS database on DMT use in patients over age 60.
MS treatment needs to adapt with advancing age for a number of reasons, Dr. Hua stated. “Older patients have less overt inflammatory disease activity,” she noted. In a retrospective Canadian study of 2,477 patients followed over a mean of 20.6 years, relapse rates decreased by 17% every five years. “As the immune system ages, factors such as oxidative injury, iron accumulation, loss of reparative mechanisms and energy efficiency, and smoldering compartmentalized CNS inflammation begin to shift the disease profile.” Older adults also have a significantly higher risk of infections, Dr. Hua added, an important factor in treatment decisions.
In her research study based on the MS PATHS database of 2,738 patients over age 60, most were not taking a DMT. Of those who were (mainly those classified as having relapsing disease), the most commonly used agents were interferons and glatiramer acetate. There remains a dearth of knowledge about the efficacy of DMT in this population and what happens when the patient goes off the therapy. Of the few discontinuation studies completed to date, most have been in younger groups of patients who stopped therapy.
Dr. Hua was the lead author of a recent study, “Discontinuation of disease-modifying therapy in patients with multiple sclerosis over age 60,” published in 2019. In this study of 178 discontinuers followed over a median of 4 years, 10.7% later reinitiated DMT, with the primary reasons cited as patient preference and clinical progression. Interestingly, only one documented relapse was recorded among those patients who discontinued therapy, and the overall cohort had limited disease activity on MRI, Dr. Hua said.
Although data are still wanting, MS clinicians still need to make decisions about DMT use in this population. Dr. Hua shared the current strategies from the Cleveland Clinic Lou Ruvo MS Center (see box).
Older, stable patients with no evidence of clinical relapse or MRI changes for past 2 yearsAge less than 60• Continue current therapy as long as patient tolerates and no safety concerns• If safety concerns (lymphopenia, JCV antibody seroconversion, increased infection rates, new or worsening comorbidities impacting DMT), switch to DMT with more favorable safety profile• If side effects become intolerable, switch to DMT with more favorable side effect profileAge greater than 60• Consider stopping DMT• Consider that co‐payments may no longer be affordable for patients who switch from commercial insurance• Monitor patients for return of disease activity after discontinuation• Consider that new T2 lesions on MRI may be vascular rather than demyelinating
To register for the Annual Meeting educational sessions, please go to:
© 2021, Consortium of Multiple Sclerosis Centers and Delaware Media Group. All rights reserved. None of the contents may be reproduced in any form without prior written permission from the publisher. The opinions expressed in this publication are those of the presenters and do not necessarily reflect the opinions or recommendations of their affiliated institutions, the publisher, or Horizon Therapeutics plc.